
By: Dave Kingsley

Narratives Make a Huge Difference in Politics: The People’s Data Project (PDP) Will Debunk the Nursing Home Industry’s False Narrative
The nursing home industry, represented in Washington, D.C. and all 50 states by the American Healthcare Association, has been successful in pushing a simple narrative: “Nursing home companies are operating on a ‘thin margin’ due to inadequate Medicaid reimbursement; therefore, they can’t afford to provide adequate staffing and decent care.” This hardship plea has been successfully sold to politicians, the media, academics, and the public in general.
At the People’s Data Project, we have the data and the data analytic tools to debunk AHCA-funded misinformation. We will begin with the misleading annual report[i] put out by the major accounting firm of Clifton, Larson, & Allen (CLA) on behalf of the industry. The bar charts below appear in the accounting firm’s latest report. These graphics display the nursing home industry “Median Operating Margin” for 2023.
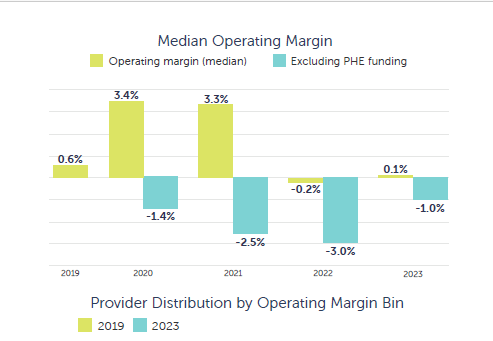
“From a financial and statistical perspective, the above presentation is highly flawed….”
From a financial and statistical perspective, this presentation is highly flawed and, for a leading accounting firm, disingenuous. We have the same data as CLA. We will show briefly in this post why the operating margin as referenced in the above graphic has no relevance to the important concept of “cash flow” – the flow of capital through a network of facilities onto the Income statements, “Cash Flow statements, and “Balance Sheets” of Parent Corporations. Rarely are nursing home facilities stand alone, independent subsidiaries with meaningful financial statements. Rather, they are conduits for cash to parent/holding companies.
The PDP data files include data from cost reports submitted by 14,440 facilities for 2023. Net operating income in our file – displayed in the table below – is not significantly different than that reported by CLA.
Certainly, accountants at CLA know that foisting these statistics in this manner on an unsuspecting public is unethical. They are failing to add data and explanations that place them in proper perspective. The data are extremely skewed in a negative direction, which pulls the average and even the median in a negative direction. A skew of -38.33 is so extreme that point estimates are of no use when all the data is dumped into a stats package and no adjustment is made for the shape of the data.

But statistical validity problems such as skew aren’t the only problems with the way nursing home operating net is used in the industry narrative. Here are the major problems with operating net that CLA accountants most certainly understand:
- Net operating income (net income from service to patients) is net patient revenue minus expenses. Expenses include payments to parent and holding companies of the facilities reporting net operating income (see the table below, which indicates $16 billion allocated to related parties and home office allocations).
- Reimbursement from sources other than Medicaid/Medicare reimbursement and self-pay are not included in operating net income. However, as the table below indicates, other revenue for state incentive programs, COVID relief, and other sources totaled $18.6 billion in 2023 but is not added to the operating margin by CLA & AHCA.
Operating expenses of $172.6 billion include payouts to parent/holding companies for management fees of $16 billion. Also, other revenue from incentive programs, COVID relief, and other sources of $18.6 billion added to the net patient revenue, along with home office allocations and payments to related parties (subsidiaries owned by parent/holding companies) creates a different perspective than operating net.
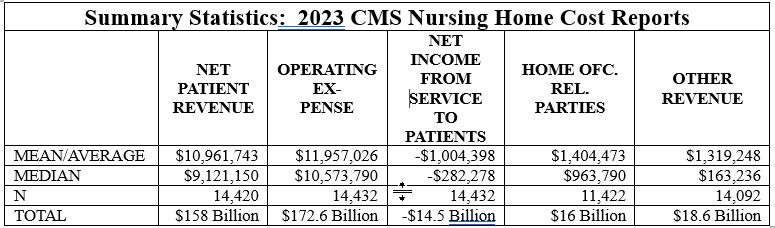
When home office allocations, payments to related parties, and nonpatient revenue is added to net operating income, it appears that 12.7% of industry patient revenue is funneled to owners of nursing home chains. There are other sources of income for chain owners through tax write-downs for interest, taxes, and depreciation. In future posts, we will discuss other vehicles available to the nursing home industry for adding value to Medicare and Medicaid reimbursement.
[i] See: Clifton, Larson, Allen (2024): The Great Divergence 39th_snf_cost_comparison_report_final.pdf