By Dave Kingsley
Don’t worry about the financial impact of COVID-19 on the nursing home industry. Corporations paid to provide long-term care appear to be doing well financially. In this post, I want to begin a discussion of the industry’s and regulators’ failure to protect patients from a scourge they should have known was coming. Unfortunately, nursing home owners are not being held accountable. Quite to the contrary, they are being financially rewarded as victims of the pandemic.
My purpose in this post is to highlight the subsidization of the industry through immediate cash infusions while nursing home personnel have been forced to work in the same low paid jobs without adequate personal protective equipment. This is an initial post in a series of posts in which I will provide information gleaned from the 2nd quarterly reports of three different types of publicly listed nursing home corporations – privately held corporations’ financial information isn’t available because they are not required to file reports with the SEC.
If the public thinks providers of nursing home corporations are financially strapped due to the COVID pandemic, they will be dissuaded from that perspective by the 2nd quarterly 10-Q reports filed by a sample of publicly listed corporations. Consider the financial reports of the following representative corporations:
The Ensign Group
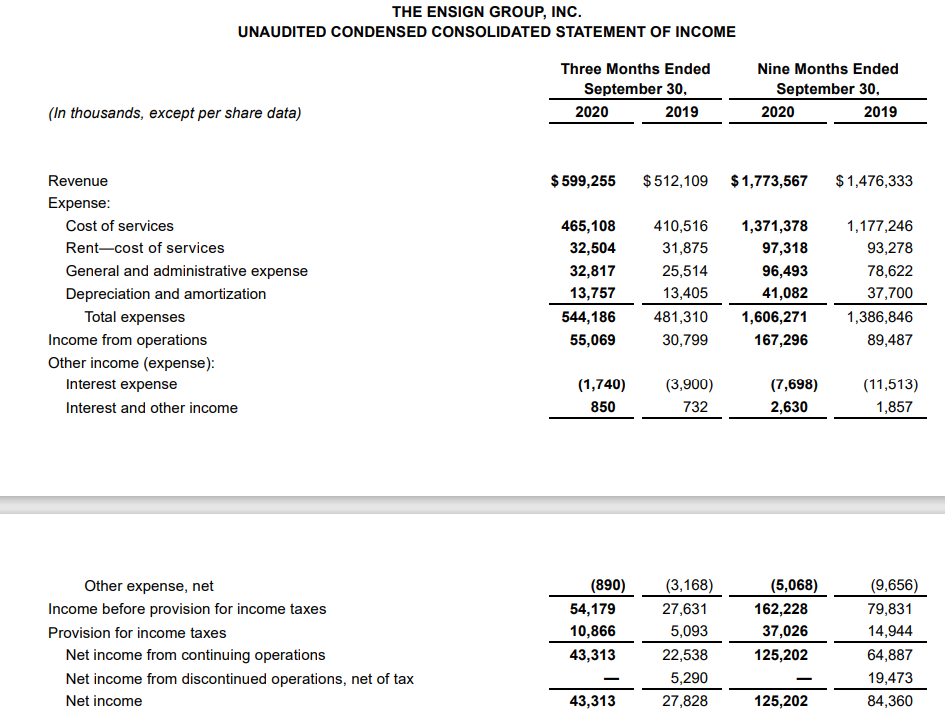
The Ensign Group, a holding company, owns the fifth largest nursing home chain in the United States. The company was formed in 1999 and, based on SEC filings, has demonstrated a robust growth and strong financial performance. According to its 2020 2nd Quarter report (10-Q)[1], its earnings of $.78 per share was a 100% increase over the prior year quarter. Revenues for the quarter were $584.7 million and increase of 18.6% over the prior year quarter. Net income for the quarter was $43.1 million, an increase of 99% over the prior year quarter.
Apparently TEG was doing so well, the corporation decided to return $110 million it received from the federal government under the CARES Act[2], which was basically a handout to America’s corporations for keeping them solvent even though nursing home companies had a guaranteed price and ongoing revenue. Furthermore, they benefitted from the Payroll Protection Program and the HEROES’ Act intended to help companies keep employees paid and enough capital to maintain solvency. Although, the TEG balance sheet indicates that the company has $210 million in cash and $302 million in accounts receivables, it still took perhaps a 100 million dollars of PPP money and a host of other CMS supplemental payments.
Ventas Real Estate Investment Trust
Ventas Real Estate Investment Trust (REIT) is illustrative of one of various types of corporations dependent on revenue from skilled nursing facilities. REIT’s in the nursing home business are a special type of commercial real estate, but they are also a special type of skilled nursing home corporation. Although they buy and lease facilities, they actually lease to contractors such as Brookdale from whom they often buy facilities and lease them back while also maintaining an interest in and control over operations. Furthermore, REITs have an operational interest in skilled nursing facilities. Ventas describes its business this way: “We primarily invest in senior housing, research and innovation, and healthcare properties through acquisitions and lease our properties to unaffiliated tenants or operate them through independent third-party managers.”
According to Ventas’s 10-Q[3], the COVID pandemic has not been financially disastrous due to the injection of funds from the CARES, PPP, and HERO’S acts.
“In our healthcare triple-net leased properties portfolio, we collected substantially all rent due in the first and second quarters. This cohort of tenants has benefitted from significant government financial support to partially offset the direct financial impact of the COVID-19 pandemic on healthcare providers. Nationally, hospital inpatient admissions and surgeries have rebounded, although still below pre-COVID-19 levels, depending on the particular market.”
Brookdale Senior Living
Brookdale Senior living is the largest operator of senior living properties. The company has sold most of its real estate.
During months ended June 30, accepted $33.5 million of cash from CARES Act. During July 2020 company applied for additional grants Emergency Funds based on 2% of portion of 2018 gross revenue from patient care
Under the CARES Act, the Company has elected to defer payment of the employer portion of social security payroll taxes incurred from March 27, 2020 to December 31, 2020. One-half of such deferral amount will become due on each of December 31, 2021 and December 31, 2022. As of June 30, 2020, the Company has deferred payment of $26.5 million of payroll taxes and presented such amount within other liabilities within the Company’s condensed consolidated balance sheet.[4]
As of June 30, 2020, total liquidity was $600.2 million, consisting of $452.4 million of unrestricted cash and cash equivalents, $109.9 million of marketable securities, and $37.9 million of additional availability on revolving credit facility.
Eric Carlson of Justice in Agency statement
Eric Carlson, of Justice in Aging served on the so-called “Independent Nursing Home COVID-19 Commission,” and was the only member who refused to endorse the commission report resulting from a series of secret meetings between July and September. I say good for him! I say shame on those other members who either fully or partially endorsed a report that allowed the Trump Administration and nursing home corporations escape responsibility for dereliction of their duty to protect nursing home patients during the COVID-19 pandemic.
Mr. Carlson gave the following reason for his refusal to endorse the report: “With limited exceptions, these recommendations … do not address accountability of nursing homes and their operators.” Having spent a considerable amount of time analyzing the report thus far, I would say that he is correct.
Not only did CMS use the report to excuse its own inept and failed response to the COVID-19 pandemic, it also ignored failure of the industry and expectations from nursing home corporations in the future. The Trump Administration failed to hold corporations accountable. Furthermore, they have been providing generous subsidies through the CARES, PPP, and HEROES Acts passed by congress in March to keep employees paid and businesses from bankruptcy.
[1] https://investor.ensigngroup.net/sec-filings/sec-filing/10-q/0001125376-20-000134
[2] Two major pieces of legislation, the CARES Act, and the HEROES Act, which include cash grants, support for employees, and deferred payroll taxes are responsible for injecting hundreds of millions of dollars into the three corporations featured in this post alone. The text of the acts can be found at: https://www.congress.gov/bill/116th-congress/senate-bill/3548/text?q=product+actualizaci%C3%B3n; https://www.congress.gov/bill/116th-congress/house-bill/6800/text. Detailed information from the income, balance sheet, and cash flow statements of major publicly listed nursing home corporations’ cash and equivalents, earnings, and liquidity indicate a rather strong financial position after several months of a nationwide pandemic.
[3] https://ventasreit.gcs-web.com/static-files/5ea1570e-14fd-45f6-8e31-15237eb49016
[4] https://brookdaleseniorlivinginc.gcs-web.com/static-files/0213cc1d-9228-4f8c-a7d4-273a1943197c