By:
Dave Kingsley
Dismantling of the Federal Administrative State
President Ronald Reagan said this at a press conference in 1986: “The nine most terrifying words in the English language are ‘I’m from the government and I’m here to help.’” This might have seemed funny at the time but by 2008 when lax federal governmental oversight of the financial services industry led to economic collapse or when in 2020 a deteriorated public health system led to a raging COVID epidemic, the people of America were screaming back to the government these five desperate words: “For God’s sake help us!”
President Reagan’s quip was a continuation and acceleration of devolution of power from the federal government to the states that began during the Nixon administration. Consequently, the far-right dream of dismantling the federal administrative state has led to funneling federal grants to states as block grants rather than grants-in-aid, which meant less federal control over how states regulated federal-state funded programs such as Medicaid and welfare in general.
Some states are more enlightened than other states in how they administer welfare programs. But during the Clinton Administration, the mistaken notion that people needing assistance for their daily needs – including medical care – would benefit from some tough love like denial of any services after a few years of receiving it. Aid to Families with Dependent Children (AFDC a grant-in-aid program) became Temporary Aid for Needy Families (TANF – a block granted program with a much more stigmatizing moniker). By the late 1990s, President Clinton was declaring that “the era of big government is over” – seven very unfortunate words.
The idea that poor people down on their luck needed some federal assistance for survival was warped into a philosophy that help from the government would induce dependency and that administrative barriers to assistance and forcing people off of aid would somehow be character building. As has happened since the era of industrialization began, poor people were more intently looked at as irresponsible and the cause of their own plight. By the turn of the Century, this philosophy had become de rigueur – even in states given to a more empathetic and compassionate approach to the less fortunate (which could be any of us).
How Have States Handled their Increasing Power?
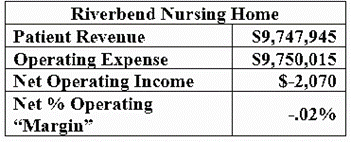
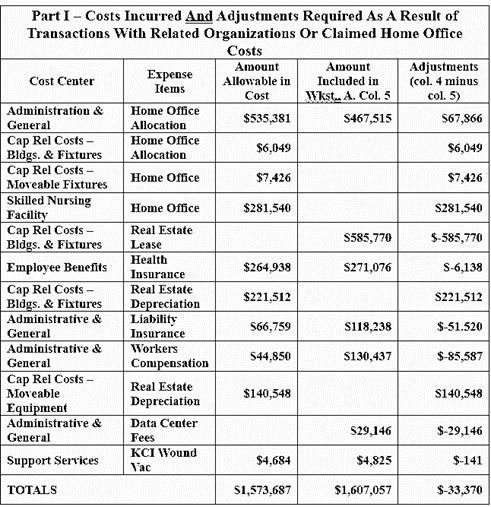
So, how have states done with the power devolved to them? Not well. As an example, consider the prior authorization of Medicaid that I wrote about in my last blog post. The HHS, OIG had this to say in their recently released report: “most State Medicaid agencies reported that they did not routinely review the appropriateness of a sample of MCO denials of prior authorization requests, and many did not collect and monitor data on these decisions.” This seems like very familiar state regulatory behavior to me. Having reviewed thousands of nursing home cost reports, I have yet to see one properly filled out (in accordance with GAAP/FSAB accounting principles and federal regulations). Indeed, they are loaded with deceit, misinformation, and what is either profound ignorance or fraud. And yet auditing at the state level appears to be practically nonexistent.
There is no point in using nursing home cost reports for research except to raise issues of state incompetence, lack of oversight capacity, and corporate ability to game the system. The same can be said about the giant insurance corporations contracting with states as MCOs. Indeed, Anthem’s highest MCO denial rate was 34%. Molina, one of the largest providers had denial rates that ranged from 17% to 41%. Aetna, Centene, and UnitedHealth denial rates were 5% to 29%, 3% to 23%, and 7% to 27% respectively.
The States with the highest rates of denial are Georgia (34%), Michigan (32%), California (29%), Mississippi (27%), New Jersey (27%), Virginia (26%), and Wisconsin (25%). One can only imagine how difficult and frustrating it is for physicians and Medicaid patients in these states to obtain needed medical care. None of these states used denial data for oversight.
There is Nothing Funny about Government Help: We Need it Badly!
My colleagues and I spend our working hours attempting to ferret out information from states regarding Medicaid outcomes data. To quote Warren Buffet, “It’s like getting red meat out of a tiger cage.” But we have been communicating with staff – including auditors – in the OIG’s office and will continue that communication. Our mission is to fight the state/federal barriers to public information.
The Medicaid program is nominally a $900 billion federal/state expenditure. But with tax expenditures (i.e., tax subsidies) for corporations in the business, it is a much larger expenditure in federal and state budgets combined than that. Furthermore, nursing home corporations and the giant insurance corporations contracting as MCOs are extracting immense amount of tax dollars without a correlative investment in a loyal, career-oriented work force, and a medical services infrastructure that welcomes and benefits the people eligible to receive it.
Centene, UnitedHealth, and the other large providers are lavishing obscene compensation packages on executives and board members (CEOs are usually receiving about $20 to $24 million per year); they have billions of dollars sitting on their balance sheets, they are paying robust dividends to their shareholders (most of which are asset managers such as Vanguard, BlackRock, and State Street, handling pension, insurance, and sovereign wealth funds); and they have devoted billions to capturing government through lax lobbying and election financing.
No matter how objective and scientific researchers like to be, this is all about politics. It’s about what goes on inside the D.C. beltway and in state capitols. Anyone who thinks they can be politically neutral, purely professional, and outside of politics is sadly mistaken. Making CMS do its job is a political task and will take political organizing. The same can be said about making state agencies do their job. You cannot work within the system and change it that way.